Introduction
Diffuse large B-cell lymphoma (DLBCL) accounts for approximately 30-50% of all non-Hodgkin’s lymphoma cases, being the most common subtype (Rovira, 2015). Every year, more than 27,000 people receive a DLBCL diagnosis in the United States of America (USA). Even though it can occur in childhood, DLBCL is more common as people age, and the majority of patients are diagnosed when they are over 60. When left untreated, DLBCL patients have a median survival of less than a year and often exhibit aggressive behavior. With 50% of patients experiencing full remissions, the CHOP regimen—cyclophosphamide, Adriamycin, vincristine, and prednisone—has been the accepted treatment since the 1970s. The addition of rituximab, the first approved anti-CD20 monoclonal antibody, to chemotherapy, also known as immunochemotherapy or R-CHOP, has significantly improved the prognosis of DLBCL over the past ten years. The most recent 5-year relative survival rate was 62.0% in the US and 55.4% in Europe (Crump, 2017). Nevertheless, 20% to 50% of DLBCL patients will either relapse after achieving a full response or be refractory to R-CHOP. These patients have a poor prognosis, particularly if they have high-risk factors. Currently, there are no curative treatment options for the majority of patients with refractory DLBCL (Crump, 2017).
One category of non-responders are patients who pass away while receiving R-CHOP induction therapy. It is frequently challenging to discern between the disease progression and death as the underlying cause. In one study (Rovira, 2015), 92 patients out of 816 (11%) died during the induction phase, with infectious complications accounting for 3.7% of patient deaths.
Presentation of the Clinical Case
Mrs D.C.P., had suffered for years with high blood pressure (treated with valsartan) and chronic antral gastritis (Helicobacter p. negative). She showed some preliminary signs of the disease in December 2015, suffered a sepsis by E. coli, and in February 2016 a right external jugular vein thrombosis (treated with low molecular weight heparin from this date until 2018). In early January 2017, (aged 77) adenopathies appeared in her lateral neck regions, which grew rapidly. She felt very tired, was in poor health and had arthralgia in several joints (Figure 1, left).


Figure 1. Mrs D.C.P. Left: February 2017. Right: April 2018
In February 2017, a PET-CT scan was performed and showed multiple adenopathies and lymph node conglomerates in several regions: both sides of the neck, supraclavicular fossa, mediastinal, along the aorta and vena cava, iliac, inguinal and mesenteric regions, with a SUVmax ranging from 6 to 25 (Figure 2, left).
An inguinal lymph node biopsy resulted in a diagnosis of diffuse large B-cell lymphoma (DLBCL), with negative CD5 and kappa light chain – diagnosed as stage IIIb. Positive immunohistochemical markers were: CD-79a, CD-20, Bcl-2, PAX-5. Negative immunohistochemical markers were: AE1-AE3, CD10, CD30, Bcl-6, CD3, CD5, CD7, MUM1, c-myc, ALK1, EBV, CD23, Cycline D1, CD15.
In late February 2017, she started 3 cycles of chemotherapy with R-CHOP (rituximab, cyclophosphamide, Adriamycin, vincristine sulfate and prednisone) through a PICC line. She reacted poorly with several hospital admissions for febrile neutropenia and even septic shock (May 2017). Due to the poor tolerance, she received another 3 cycles of R-COP (without Adriamycin), with the last cycle administered in July 2017. The patient did not tolerate this regime and her general state of health worsened. In consultation with her hematologist and family, the patient decided to stop all chemotherapy.
A PET-CT scan performed 40 days after the last chemotherapy cycle revealed that some previously positive lymph nodes have disappeared, some have persisted, and some had increased their glucose uptake: right lateral cervical region (SUVmax 2.54), left lateral cervical region (SUVmax 2.21), right supraclavicular fossa (SUVmax 2.08), mediastinal (SUVmax 4.79), mesenteric (several adenopathies, with a new glucose uptake focus adjacent to the descending colon, with a SUVmax of 7.78). The diagnostic conclusion provided by the radiologist was that of “metabolic progression”.
In December 2017, patient Mrs. D.C.P., was in very poor health, very tired, without appetite, apathic and cold. The treatment with our protocol using alpha-lipoic acid, vitamin C, vitamin D, selenium and ozone started on this date, as will be described in later sections.
Materials and Methods
Mrs. D.C.P. was an out-of-town patient and came for IV treatment a total of 10 times, with a mean of 6 days each time, for a period of 1 year and 5 months, starting December 2017 until April 2019 (see Table 1).
A typical day of IV treatment consisting of 50 grams of sodium ascorbate (with magnesium sulfate) in 500 cc of sterile water, infused at approximately 1 gram every 2 minutes. This was followed by the infusion of 300 mg of alpha Lipoic acid (ALA) from ASTA, in 100 cc of saline over 40-45 minutes. Afterwards, an infusion of 5 to 10 mg of sodium selenite with 30 mg each of vitamins B1 and B6, 500 mcg of hydroxocobalamin, 350 mcg of methylcobalamin, and an addition of trace minerals (Manganese 0.18 mg, Zinc 0.29 mg, Copper 0.5 mg, Magnesium 50 mg, Potassium 50 mg), in 100 cc of saline, was infused over 45 minutes. At the end of the morning, a portable pump with 300 mg of ALA diluted till 20 cc in saline was applied to the PICC line, to be infused continuously over 20-24 hours.
On alternate days, in the afternoon there was high-dose ozone therapy (HDOT) with multiple passes. This is a technique pioneered and developed by Dr. Johann Lahodny (St. Pölten, Austria) and each “pass” consists of combining 200 cc of patient´s blood in a 250 cc glass bottle (Zotzmann and Stahl) with 700 IU of heparin, then infused with 200 cc of ozone at 70 mcg/ml in the bottle under hyperbaric pressure (1 bar). This is mixed with the blood and re-infused back into the patient. The treatment could be repeated in the same session several times, typically 10 times (referred to as HBOT, 10 pass or L1). The ozone gas was produced from medical oxygen in a Zotzmann Ozon 2000 machine.
All the infusions including those delivered using the portable pump, were infused through her PICC line, using strict sterile technique, and with the application of 5 ml of a 20 IU/ml heparin lock when not in use. The high-dose ozone therapy was done with a 19G butterfly needle in one of her antecubital fossa veins.
Orally administered treatments included:
- Vitamin D: from December 2017 until April 2018: 60,000 IU per day (prepared by a compounding pharmacy). Parathyroid hormone was controlled to be not less than 20 pg/ml (normal range: 14-100) and serum calcium did not go beyond 10.5 mg/dL (range: 8-10.5). Serum 25(OH)vitamin D would range from 90-160 ng/ml. This high-dose vitamin D is based on a protocol developed by Dr. Cicero Coimbra in Sao Paulo, Brasil, obtained through personal communication. After April 2019, we lowered the dose to 20,000 IU per day, and later to 5,000 IU/day
- Low-dose naltrexone (LDN): 3 mg per day in the evening.
- Alpha-Lipoic acid (ALA): 300 mg tablet every 12 hours (when not receiving IV ALA)
- Selenium (Se), as Se-Methyl L-Selenocysteine: 200 mcg every 12 hours. (when not receiving IV Se)
- Milk thistle extract, providing 480 mg silymarin, 180 mg silybin, 48 mg isosilybin A and isosilybin B (700 mg): one capsule every 8 hours.
- B-complex 50 (Solgar): once or twice a day.
- Probiotics: commercial preparation of 25×109 containing: Lactobacillus acidophilus, Bifidobacterium bifidum, Bifidobacterium animalis subsp lactis taken every 12 hours, plus 108 of Lactobacillus reuteri once a day. Fresh fermented food, such as kefir and sauerkraut were included in her diet.
- Dietary modification was not very strict, as we feel that has the potential to diminish quality of life and produce stress in the patient. Guidelines included some amount of fresh juices made of organic carrots, apples, green leaves and fresh curcuma roots. For breakfast, boiled oats with fresh fruits, and for lunch and dinner salads, steamed vegetables and soups. She was advised to avoid fried food and dry or preserved meats. Once a week the patient could have a small amount of animal protein including fish or meat.
We tried to avoid any infectious foci anywhere in the body, because the cytokines produced in these foci might encourage B-cell growth. In this sense, we ordered a dental CT scan, that revealed an infectious focus, that could not be seen in normal X rays. This was repaired. We also advised to avoid any stress that could negatively impact her healing.
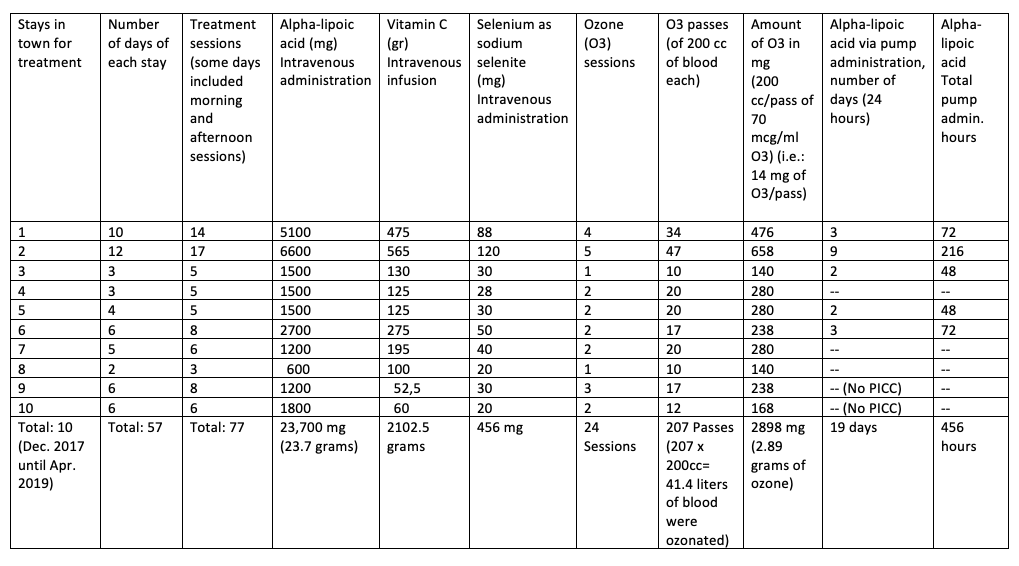
Table 1. Treatment schedule and nutrient amounts used.
Result
Mrs. D.C.P. slowly regained her health, and after a few months she declared “I feel normal again” (Figure 1, right). Lymph nodes progressively disappeared, although she would complain that some nodes were “appearing and disappearing” in her abdominal wall.
There were almost no side effects from this treatment. Only once she had a hypoglycemic event with shaking and a cold feeling. That was resolved by infusing some 5% glucose and eating a piece of fruit.
Interestingly, her blood pressure normalized and she stopped valsartan treatment, probably due to vitamin D (Rai & Agrawal, 2017) and ozone (Juchniewicz & Lubkowska, 2020).
In April 2019, 1 year and 5 months after starting this program, she felt well enough to continue with her normal life again and the IV program was discontinued and replaced with the oral supplement regime only.
In August 2019, a control CT scan reported “there are no morphological signs that could suggest a lymphoproliferative condition”
At the beginning of summer 2020, she felt unusually tired. Her hematologist was afraid that she had relapsed from her lymphoma. A PET-CT scan was obtained in August 2020 (See Figure 2, right), and the radiologist reported that the “PET-CT scan with 18F-FDG demonstrated no metabolic evidence of malignancy”. So, the tiredness was due to something else, and eventually resolved by itself.
As of December 2024, the patient continues to be symptom-free. She has not received any further IV treatment for her lymphoma since April 2019 (i.e. more than 5 years).


Figure 2. PET-CT images. Left: 2017. Right: 2020.
Discussion
Alpha-Lipoic Acid
Alpha-lipoic acid (ALA) was the first essential element in the patient’s treatment regimen. Compared to the oral form, intravenous ALA can achieve significantly higher plasma levels. Oral capsules were used to sustain levels between IV infusions (Berkson, 2006). The positive result in this instance can be attributed, at least in part, to the wide range mechanisms of action of ALA. For example, it is a potent antioxidant and heavy metal chelator (Gorąca, 2011). However, we believe that three of its effects—its anti-inflammatory properties, its significant impact on mitochondrial metabolism, and its ability to modify epigenetics—are more pertinent in this instance (Berkson & Calvo Riera, 2018).
ALA may inhibit the growth of cancer cells through its interaction with nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB), a pro-inflammatory transcription factor (Ying, 2011). In addition to making malignant cells resistant to apoptosis, unchecked NF-kB activation can cause angiogenesis, mutagenesis, metastasis, proliferation, and chemo-radio resistance (Pavitra, 2023). Due in part to NF-kB activation, patients with advanced cancer have significantly higher levels of oxidative stress markers and an ongoing inflammatory processes (Pavitra, 2023). By inhibiting NF-kB, ALA lessens these harmful effects and may help reduce cancer cell growth.
Another significant interaction of ALA is with the pyruvate dehydrogenase enzyme (PDH) and its regulatory enzyme pyruvate dehydrogenase kinase (PDK). PDH consists of three mitochondrial enzymes located in the convergence of cytoplasm and mitochondria, glycolysis and the Krebs cycle, and anaerobic and aerobic metabolism. Pyruvate produced in the cytoplasm is metabolized by PDH into acetyl-CoA, which subsequently enters the Krebs cycle. ALA is a necessary cofactor for PDH, and in the absence of ALA the energy production of the mitochondria is severely impaired (Berkson & Calvo Riera, 2018).
PDK controls the activity of PDH by phosphorylating and inhibiting it. In addition to being the PDH essential cofactor, ALA also inhibits PDK, which increases PDH activity even more (Patel & Packer, 2008; Korotchkina, 2004).
These enzymes play a part in the so-called Warburg effect, also known as “aerobic glycolysis,” a metabolic peculiarity of cancer cells that is rather common to malignancies: even when oxygen is present, cancer cells preferentially metabolize glucose and pyruvate into lactic acid (Warburg, 1956). The production of amino acid and nucleotide precursors, which are crucial for a cell that is proliferating quickly, may be favored by this increase in glycolysis, potentially offsetting the drawback of decreased ATP production (DeBerardinis, 2008; Vander Heiden, 2009).
Inhibition of PDH activity has been demonstrated by McFate et al. (2008), to contribute to the Warburg metabolic and malignant phenotype. This inhibition was brought on by increased PDK expression. PDK knockdown reduced invasiveness, inhibited the growth of xenograft tumors, restored PDH activity, and reversed the Warburg metabolic phenotype.
Hypoxia inducible factor-1 (HIF-1) is constitutively up-regulated in many tumors. Because HIF-1 activates PDK, one of its target genes, with subsequent PDH inhibition (Kim, 2006), it promotes the Warburg effect in a number of cancers (Semenza, 2007).
In essence, ALA has the potential to alter the metabolic shifts that are characteristic of cancer cells (specifically the Warburg effect) by inhibiting PDK and activating PDH, pushing metabolism back toward mitochondrial oxidative phosphorylation. This shift would reduce the reliance on glycolysis and could destabilize the cancer cell’s growth program thereby interfering with the metabolic reprogramming that supports rapid tumor growth, making it less efficient and potentially more vulnerable to treatments.
ALA’s ability to modify epigenetics is another possible antitumor effect. PDH, which was previously believed to be a mitochondrial enzyme, has recently been discovered to be present and functional in the nucleus, most likely translocated from the mitochondrion (Sutendra, 2014). Histone lysine residue acetylation was reduced in isolated nuclei when nuclear PDH was inhibited. Since lipoic acid is also a cofactor for this nuclear PDH, ALA offers a source for the synthesis of nuclear acetyl-CoA, which is necessary for histone acetylation and epigenetic control. ALA not only provides the acetyl-CoA for histone acetylation, but also inhibits certain histone deacetylases (Lechner, 2023). Acetylation and deacetylation of histones are crucial elements in the regulation of genes.
In recent years, the connection between epigenetics and cancer has drawn a lot of attention. Without changing the underlying genetic code, epigenetic changes like DNA methylation, histone modification, and non-coding RNA regulation can affect how genes are expressed. Important cellular functions that are essential to tumorigenesis, such as growth, apoptosis, and metastasis, may be impacted by these alterations (Yu, 2024).
There is a growing view that cancer is a metabolic disease in addition to a genetic one. ALA seems to have a dual mechanism of action, potentially targeting both the metabolic and genetic aspects of cancer.
Berkson and Calvo-Riera used alpha-lipoic acid in a number of cancer cases, which led to long-term remissions (Berkson, 2006; Berkson, 2007; Berkson, 2009; Berkson & Calvo Riera, 2018; Berkson & Calvo Riera, 2021).
Vitamin C
The patient’s treatment regimen also included intravenous vitamin C. For many years, cutting-edge medical professionals have used this agent, with a number of encouraging case studies (Mikirova, 2013). These outcomes include slowing down the PSA doubling time in prostate cancer (Tareen, 2008), and reversing pulmonary metastases from hepatocellular carcinoma and renal cell carcinoma (Sao, 2015; Fritz, 2014).
High-dose IV vitamin C may have anticancer effects because its action at many different levels: it lowers inflammatory biomarkers in cancer patients, including interleukins IL-1, IL2, IL-6, and IL-8, C-reactive protein (CRP), tumor necrosis factor (TNF-α), and interferon-γ (IFN-γ) (Mikirova, 2008; Jafari, 2019). Using human leukemia cell lines, other authors demonstrated that vitamin C suppresses the growth of human leukemic cells by downregulating HIF-1α (Kawada, 2013). Angiogenesis, the epithelial-mesenchymal transition (EMT), stem cell maintenance, invasion, metastasis, and resistance to chemotherapy and radiation therapy are all mediated by HIF activity (Semenza, 2012).
Studies on animals and in vitro have demonstrated that high doses of vitamin C cause pro-oxidant effects and specifically destroy cancer cells (Chen, 2005). It encourages ferroptosis (Wu, 2024), a form of cell death, through its interaction with intracellular iron.
Selenium
As present in selenoproteins such as selenocysteine, selenium is commonly recognized as an antioxidant; However, depending on concentration and chemical species, selenium can produce a cytotoxic oxidative stress in cancer cells (Misra, 2015; Brodin, 2015), as well as ferroptosis (Choi, 2023).
Ozone Therapy
Ozone therapy’s pleiotropic effect and its anti-inflammatory, oxidative stress-inducing, and immunomodulatory qualities have made it a promising adjunctive treatment for various cancer types (Fetner, 1958; Baeza-Noci & Pinto-Bonilla, 2021; Perez Olmedo, 2024, Pryor, 1991). Additionally, ozone has been implicated in the peroxidation of polyunsaturated fatty acids, which has been identified as a major cause of oxidative damage to cellular membranes that results in cell death, likely via ferroptosis (Li & Pu, 2024; Pryor, 1991).
Vitamin D
Vitamin D is a hormone produced by the skin in response to sunlight. It has been shown to play a role in immune system regulation. The following discovery has further established vitamin D’s role in immune system regulation: Vitamin D receptors (VDRs) are found in nearly all immune system cells and play an important role in both adaptive and innate immune responses (Hewison, 2011). Induced VDR has been shown to inhibit NF-κB activation and reduce inflammation (Bikle, 2009).
Vitamin D has been shown to inhibit carcinogenesis by inducing cellular differentiation, inhibiting proliferation and angiogenesis, and promoting apoptosis (Chakraborti, 2011). Notably, it has been demonstrated that vitamin D inhibits the proliferation of lymphocytes and lymphoma cell lines and induces their differentiation in vitro (Bikle, 2009; Hickish, 1993).
Patients with diffuse large B-cell lymphoma (DLBCL) who were 25(OH) vitamin D deficient were found to have a lower overall survival rate (Drake, 2010).
All agents described above have multiple, pleiotropic, activities and we believe that there might have been a synergistic and complementary interaction between all these different activities, providing a more comprehensive therapeutic effect.
Conclusion
Here we have described a comparatively non-toxic cancer treatment protocol that has changed the life of a very ill woman who had a diffuse large B cell lymphoma to that of someone free of this potentially fatal disease.
The combination of lipoic acid, vitamin C, selenium, vitamin D and ozone in orthomolecular doses may provide a comprehensive and synergistic therapeutic approach by targeting multiple pathways involved in oxidative stress, mitochondrial function, immune modulation, epigenetics, inflammation and ferroptosis.
We propose that such a treatment or a similar one could provide an alternative in cases where chemotherapy is not well tolerated and has to be halted. It remains to be explored if these treatments could be a possibility in cases of chemotherapy failure, or even as a first line treatment in cases of slow cancers or in frail or aged patients.
Acknowledgements
Burton Berkson, MD, PhD, died on March 4, 2024. He was a great teacher, a great doctor and a great human being.
F.C.R. thanks Dr. Ron Hunninghake for enabling a stay at the Riordan Clinic (Wichita, Kansas) and for his contribution to establishing the Riordan Clinic IV Vitamin C protocol.
Ethics
Ethics approval was not required, as this article reflects patient´s clinical treatment. The patient gave informed consent for both, her treatment and this publication.
Conflict of Interest Disclosure
All authors declare that they have no conflicts of interest.
References
Baeza-Noci, J., & Pinto-Bonilla, R. (2021). Systemic Review: Ozone: A Potential New Chemotherapy. International Journal of Molecular Sciences, 22(21), 11796. https://doi.org/10.3390/ijms222111796
Berkson, B. M., & Calvo Riera, F. (2018). The Long-Term Survival of a Patient With Stage IV Renal Cell Carcinoma Following an Integrative Treatment Approach Including the Intravenous α-Lipoic Acid/Low-Dose Naltrexone Protocol. Integrative Cancer Therapies, 17(3), 986–993. https://doi.org/10.1177/1534735417747984
Berkson B.M., & Calvo Riera, F. (2021). A Review of the Integrative Treatment Approach Using the Intravenous Alpha-Lipoic Acid/Low Dose Naltrexone (ALA/N) Protocol for Cancer and a Description of the Long-Term Survival of a Woman with Hepatocellular Carcinoma. Clinics in Oncology, 6(1), 1785.
Berkson, B. M., Rubin, D. M., & Berkson, A. J. (2006). The long-term survival of a patient with pancreatic cancer with metastases to the liver after treatment with the intravenous alpha-lipoic acid/low-dose naltrexone protocol. Integrative Cancer Therapies, 5(1), 83–89. https://doi.org/10.1177/1534735405285901
Berkson, B. M., Rubin, D. M., & Berkson, A. J. (2007). Reversal of signs and symptoms of a B-cell lymphoma in a patient using only low-dose naltrexone. Integrative Cancer Therapies, 6(3), 293–296. https://doi.org/10.1177/1534735407306358
Berkson, B. M., Rubin, D. M., & Berkson, A. J. (2009). Revisiting the ALA/N (alpha-lipoic acid/low-dose naltrexone) protocol for people with metastatic and nonmetastatic pancreatic cancer: A report of 3 new cases. Integrative Cancer Therapies, 8(4), 416–422. https://doi.org/10.1177/1534735409352082
Bikle, D. (2009). Nonclassic actions of vitamin D. The Journal of Clinical Endocrinology and Metabolism, 94(1), 26–34. https://doi.org/10.1210/jc.2008-1454
Brodin, O., Eksborg, S., Wallenberg, M., Asker-Hagelberg, C., Larsen, E. H., Mohlkert, D., Lenneby-Helleday, C., Jacobsson, H., Linder, S., Misra, S., & Björnstedt, M. (2015). Pharmacokinetics and Toxicity of Sodium Selenite in the Treatment of Patients with Carcinoma in a Phase I Clinical Trial: The SECAR Study. Nutrients, 7(6), 4978–4994. https://doi.org/10.3390/nu7064978
Chakraborti, C. K. (2011). Vitamin D as a promising anticancer agent. Indian Journal of Pharmacology, 43(2), 113–120. https://doi.org/10.4103/0253-7613.77335
Chen, Q., Espey, M. G., Krishna, M. C., Mitchell, J. B., Corpe, C. P., Buettner, G. R., Shacter, E., & Levine, M. (2005). Pharmacologic ascorbic acid concentrations selectively kill cancer cells: Action as a pro-drug to deliver hydrogen peroxide to tissues. Proceedings of the National Academy of Sciences of the United States of America, 102(38), 13604–13609. https://doi.org/10.1073/pnas.0506390102
Choi, J.-A., Lee, E. H., Cho, H., & Kim, J.-H. (2023). High-Dose Selenium Induces Ferroptotic Cell Death in Ovarian Cancer. International Journal of Molecular Sciences, 24(3), 1918. https://doi.org/10.3390/ijms24031918
Crump, M., Neelapu, S. S., Farooq, U., Van Den Neste, E., Kuruvilla, J., Westin, J., Link, B. K., Hay, A., Cerhan, J. R., Zhu, L., Boussetta, S., Feng, L., Maurer, M. J., Navale, L., Wiezorek, J., Go, W. Y., & Gisselbrecht, C. (2017). Outcomes in refractory diffuse large B-cell lymphoma: Results from the international SCHOLAR-1 study. Blood, 130(16), 1800–1808. https://doi.org/10.1182/blood-2017-03-769620
DeBerardinis, R. J., Lum, J. J., Hatzivassiliou, G., & Thompson, C. B. (2008). The biology of cancer: Metabolic reprogramming fuels cell growth and proliferation. Cell Metabolism, 7(1), 11–20. https://doi.org/10.1016/j.cmet.2007.10.002
Drake, M. T., Maurer, M. J., Link, B. K., Habermann, T. M., Ansell, S. M., Micallef, I. N., Kelly, J. L., Macon, W. R., Nowakowski, G. S., Inwards, D. J., Johnston, P. B., Singh, R. J., Allmer, C., Slager, S. L., Weiner, G. J., Witzig, T. E., & Cerhan, J. R. (2010). Vitamin D insufficiency and prognosis in non-Hodgkin’s lymphoma. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 28(27), 4191–4198. https://doi.org/10.1200/JCO.2010.28.6674
Fetner, R. H. (1958). Chromosome breakage in Vicia faba by ozone. Nature (London); (United Kingdom), 181:4607. https://doi.org/10.1038/181504a0
Fritz, H., Flower, G., Weeks, L., Cooley, K., Callachan, M., McGowan, J., Skidmore, B., Kirchner, L., & Seely, D. (2014). Intravenous Vitamin C and Cancer: A Systematic Review. Integrative Cancer Therapies, 13(4), 280–300. https://doi.org/10.1177/1534735414534463
Gorąca, A., Huk-Kolega, H., Piechota, A., Kleniewska, P., Ciejka, E., & Skibska, B. (2011). Lipoic acid—Biological activity and therapeutic potential. Pharmacological Reports: PR, 63(4), 849–858. https://doi.org/10.1016/s1734-1140(11)70600-4
Hewison, M. (2011). Vitamin D and innate and adaptive immunity. Vitamins and Hormones, 86, 23–62. https://doi.org/10.1016/B978-0-12-386960-9.00002-2
Hickish, T., Cunningham, D., Colston, K., Millar, B. C., Sandle, J., Mackay, A. G., Soukop, M., & Sloane, J. (1993). The effect of 1,25-dihydroxyvitamin D3 on lymphoma cell lines and expression of vitamin D receptor in lymphoma. British Journal of Cancer, 68(4), 668–672. https://doi.org/10.1038/bjc.1993.406
Jafari, D., Esmaeilzadeh, A., Mohammadi-Kordkhayli, M., & Rezaei, N. (2019). Vitamin C and the Immune System. In Mahmoudi, M., Rezaei, N. (Eds.), Nutrition and Immunity (pp. 81–102) Springer Cham. https://doi.org/10.1007/978-3-030-16073-9_5
Kawada, H., Kaneko, M., Sawanobori, M., Uno, T., Matsuzawa, H., Nakamura, Y., Matsushita, H., & Ando, K. (2013). High concentrations of L-ascorbic acid specifically inhibit the growth of human leukemic cells via downregulation of HIF-1α transcription. PloS One, 8(4), e62717. https://doi.org/10.1371/journal.pone.0062717
Korotchkina, L. G., Sidhu, S., & Patel, M. S. (2004). R-lipoic acid inhibits mammalian pyruvate dehydrogenase kinase. Free Radical Research, 38(10), 1083–1092. https://doi.org/10.1080/10715760400004168
Lechner, S., Steimbach, R. R., Wang, L., Deline, M. L., Chang, Y.-C., Fromme, T., Klingenspor, M., Matthias, P., Miller, A. K., Médard, G., & Kuster, B. (2023). Chemoproteomic target deconvolution reveals Histone Deacetylases as targets of (R)-lipoic acid. Nature Communications, 14(1), 3548. https://doi.org/10.1038/s41467-023-39151-8
Li, Y., & Pu, R. (2024). Ozone Therapy for Breast Cancer: An Integrative Literature Review. Integrative Cancer Therapies, 23, 15347354241226667. https://doi.org/10.1177/15347354241226667
McFate, T., Mohyeldin, A., Lu, H., Thakar, J., Henriques, J., Halim, N. D., Wu, H., Schell, M. J., Tsang, T. M., Teahan, O., Zhou, S., Califano, J. A., Jeoung, N. H., Harris, R. A., & Verma, A. (2008). Pyruvate dehydrogenase complex activity controls metabolic and malignant phenotype in cancer cells. The Journal of Biological Chemistry, 283(33), 22700–22708. https://doi.org/10.1074/jbc.M801765200
Mikirova, N. A., Ichim, T. E., & Riordan, N. H. (2008). Anti-angiogenic effect of high doses of ascorbic acid. Journal of Translational Medicine, 6, 50. https://doi.org/10.1186/1479-5876-6-50
Misra, S., Boylan, M., Selvam, A., Spallholz, J. E., & Björnstedt, M. (2015). Redox-active selenium compounds—From toxicity and cell death to cancer treatment. Nutrients, 7(5), 3536–3556. https://doi.org/10.3390/nu7053536
Patel, M. S., & Packer, L. (2008). Pyruvate Dehydrogenase Complex Regulation and Lipoic Acid. In Patel, M. S., & Packer, L. (Eds.), Lipoic Acid: Energy Production, Antioxidant Activity, and Health Effects (pp. 173–190). CRC Press. https://doi.org/10.1201/9781420045390-13
Pavitra, E., Kancharla, J., Gupta, V. K., Prasad, K., Sung, J. Y., Kim, J., Tej, M. B., Choi, R., Lee, J.-H., Han, Y.-K., Raju, G. S. R., Bhaskar, L., & Huh, Y. S. (2023). The role of NF-κB in breast cancer initiation, growth, metastasis, and resistance to chemotherapy. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie, 163, 114822. https://doi.org/10.1016/j.biopha.2023.114822
Perez Olmedo, J.C., III Congreso Mundial de Ozonoterapia. Pontevedra, Spain, 2024
Pryor, W. A., Das, B., & Church, D. F. (1991). The ozonation of unsaturated fatty acids: Aldehydes and hydrogen peroxide as products and possible mediators of ozone toxicity. Chemical Research in Toxicology, 4(3), 341–348. https://doi.org/10.1021/tx00021a014
Rovira, J., Valera, A., Colomo, L., Setoain, X., Rodríguez, S., Martínez-Trillos, A., Giné, E., Dlouhy, I., Magnano, L., Gaya, A., Martínez, D., Martínez, A., Campo, E., & López-Guillermo, A. (2015). Prognosis of patients with diffuse large B cell lymphoma not reaching complete response or relapsing after frontline chemotherapy or immunochemotherapy. Annals of Hematology, 94(5), 803–812. https://doi.org/10.1007/s00277-014-2271-1
Semenza, G. L. (2007). HIF-1 mediates the Warburg effect in clear cell renal carcinoma. Journal of Bioenergetics and Biomembranes, 39(3), 231–234. https://doi.org/10.1007/s10863-007-9081-2
Semenza, G. L. (2012). Hypoxia-inducible factors: Mediators of cancer progression and targets for cancer therapy. Trends in Pharmacological Sciences, 33(4), 207–214. https://doi.org/10.1016/j.tips.2012.01.005
Seo, M.-S., Kim, J.-K., & Shim, J.-Y. (2015). High-Dose Vitamin C Promotes Regression of Multiple Pulmonary Metastases Originating from Hepatocellular Carcinoma. Yonsei Medical Journal, 56(5), 1449–1452. https://doi.org/10.3349/ymj.2015.56.5.1449
Sutendra, G., Kinnaird, A., Dromparis, P., Paulin, R., Stenson, T. H., Haromy, A., Hashimoto, K., Zhang, N., Flaim, E., & Michelakis, E. D. (2014). A nuclear pyruvate dehydrogenase complex is important for the generation of acetyl-CoA and histone acetylation. Cell, 158(1), 84–97. https://doi.org/10.1016/j.cell.2014.04.046
Tareen, B., Summers, J. L., Jamison, J. M., Neal, D. R., McGuire, K., Gerson, L., & Diokno, A. (2008). A 12 week, open label, phase I/IIa study using apatone for the treatment of prostate cancer patients who have failed standard therapy. International Journal of Medical Sciences, 5(2), 62–67. https://doi.org/10.7150/ijms.5.62
Vander Heiden, M. G., Cantley, L. C., & Thompson, C. B. (2009). Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science (New York, N.Y.), 324(5930), 1029–1033. https://doi.org/10.1126/science.1160809
Warburg, O. (1956). On the origin of cancer cells. Science (New York, N.Y.), 123(3191), 309–314. https://doi.org/10.1126/science.123.3191.309
Wu, K., Liu, L., Wu, Z., Huang, Q., Zhou, L., Xie, R., & Wang, M. (2024). Ascorbic acid induces ferroptosis via STAT3/GPX4 signaling in oropharyngeal cancer. Free Radical Research, 58(2), 117–129. https://doi.org/10.1080/10715762.2024.2320396
Ying, Z., Kampfrath, T., Sun, Q., Parthasarathy, S., & Rajagopalan, S. (2011). Evidence that α-lipoic acid inhibits NF-κB activation independent of its antioxidant function. Inflammation Research: Official Journal of the European Histamine Research Society … [et Al.], 60(3), 219–225. https://doi.org/10.1007/s00011-010-0256-7
Yu, X., Zhao, H., Wang, R., Chen, Y., Ouyang, X., Li, W., Sun, Y., & Peng, A. (2024). Cancer epigenetics: From laboratory studies and clinical trials to precision medicine. Cell Death Discovery, 10(1), 28. https://doi.org/10.1038/s41420-024-01803-z