.
Introduction
Metabolic dysfunction–associated steatotic liver disease (MASLD), previously termed non‑alcoholic fatty liver disease, is the hepatic manifestation of metabolic syndrome and is strongly associated with obesity, insulin resistance, dyslipidemia, and type 2 diabetes mellitus (Powell et al., 2021; Younossi et al., 2016). Global prevalence estimates suggest that MASLD affects approximately one quarter of the adult population and represents one of the most rapidly increasing causes of chronic liver disease worldwide (Powell et al., 2021; Younossi et al., 2016).
The progression of MASLD from simple steatosis to steatohepatitis and fibrosis reflects complex interactions among metabolic, inflammatory, and oxidative mechanisms. Insulin resistance promotes hepatic lipogenesis and impairs fatty‑acid oxidation, leading to triglyceride accumulation within hepatocytes. Lipotoxic intermediates, mitochondrial dysfunction, and reactive oxygen species generation subsequently promote hepatocellular injury and activation of hepatic stellate cells responsible for extracellular matrix deposition and fibrogenesis (Begriche et al., 2013; Friedman, 2008; Tilg et al., 2021).
Weight reduction and improvement in insulin sensitivity remain the most widely recognized interventions associated with improvement in MASLD (Powell et al., 2021). However, reversal of advanced fibrosis is inconsistently observed and often requires substantial metabolic recovery (Armstrong et al., 2016). In metabolic liver disease the orthomolecular medicine framework includes supporting mitochondrial metabolism, maintaining membrane phospholipid integrity, correcting micronutrient insufficiencies, and reducing oxidative stress (Ames, 2006; Begriche et al., 2013; Zeisel, 2012).
This report describes regression of advanced hepatic fibrosis in a patient with MASLD treated with an integrated orthomolecular and metabolic rehabilitation strategy.
Case Presentation
A 58‑year‑old male presented with newly diagnosed type 2 diabetes mellitus accompanied by fatigue, reduced exercise tolerance, and metabolic instability. Medical history included long‑standing obesity and dyslipidemia consistent with metabolic syndrome (see Table 1 for all of the patient’s baseline clinical metrics). Alcohol consumption was minimal and there was no history of viral hepatitis, autoimmune liver disease, or exposure to hepatotoxic medications.
Baseline laboratory evaluation demonstrated severe hyperglycemia with HbA1c of 10.2% and fasting glucose of 12.7 mmol/L. Lipid profile revealed elevated total cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides consistent with insulin resistance.
Transient elastography (FibroScan) demonstrated liver stiffness of 13.5 kPa corresponding to advanced hepatic fibrosis (F3) with severe steatosis. Baseline body weight was 283 lb with a body mass index of 39.5 kg/m².
Table 1. Baseline Clinical Metrics

Treatment Protocol
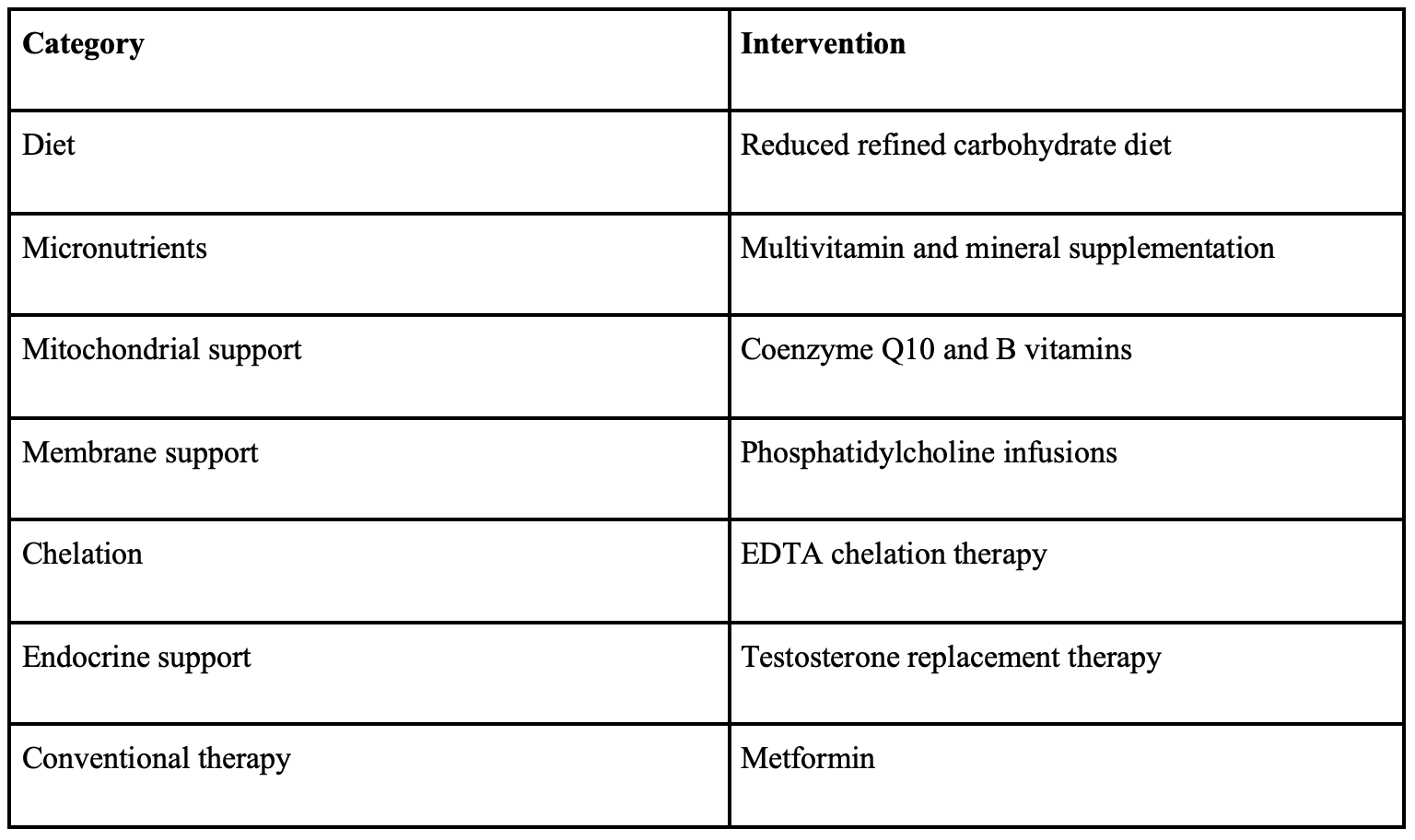
A comprehensive metabolic rehabilitation program was initiated incorporating dietary modification, progressive weight reduction, orthomolecular micronutrient therapy, intravenous nutrient infusions, phosphatidylcholine therapy, endocrine optimization, and conventional pharmacotherapy with metformin (Table 2).
Dietary modification emphasized reduction of refined carbohydrates and caloric moderation to improve insulin sensitivity and facilitate gradual weight reduction. Oral orthomolecular therapy included broad micronutrient support designed to restore enzymatic cofactors required for mitochondrial metabolism and antioxidant defense systems.
Intravenous nutrient therapy incorporated magnesium, B‑complex vitamins, and antioxidant support. Phosphatidylcholine infusions were utilized to support hepatocyte membrane integrity and lipid export mechanisms. Phosphatidylcholine is required for assembly and secretion of very‑low‑density lipoproteins responsible for transporting triglycerides out of hepatocytes (van der Veen et al., 2017).
Ethylenediaminetetraacetic acid (EDTA) chelation therapy was implemented as part of the orthomolecular program. Transition metals such as iron can catalyze hydroxyl radical formation through the Fenton reaction. In this reaction ferrous iron reacts with hydrogen peroxide to generate hydroxyl radicals capable of initiating lipid peroxidation and cellular injury within hepatocytes (Day & James, 1998). Chelation reduces redox‑active transition metals capable of catalyzing hydroxyl radical formation, thereby reducing oxidative stress.
Table 2. Comprehensive Metabolic Rehabilitation Program
Results
At baseline in July 2024 laboratory evaluation demonstrated hepatocellular injury with alanine aminotransferase (ALT) 90 U/L and aspartate aminotransferase (AST) 48 U/L, with gamma-glutamyl transferase (GGT) 55 U/L. Glycemic control was markedly abnormal with hemoglobin A1c of 10.2%. Dyslipidemia was also present, including triglycerides of 3.84 mmol/L and HDL cholesterol of 0.87 mmol/L.
Following implementation of metabolic and orthomolecular interventions, progressive improvement was observed. Over approximately twelve months, the patient experienced substantial metabolic improvement accompanied by normalization of biochemical markers of hepatic injury and regression of hepatic fibrosis. Body weight decreased from 283 lb at presentation to 216 lb at the most recent follow-up.
Hemoglobin A1c (HbA1c) declined from 10.2% to 5.9% within four months and remained in the non-diabetic range thereafter. Liver enzymes normalized during follow-up, with ALT declining from 90 U/L at baseline to 27 U/L within four months and measuring 20 U/L at the most recent follow-up. AST and GGT also normalized during follow-up.
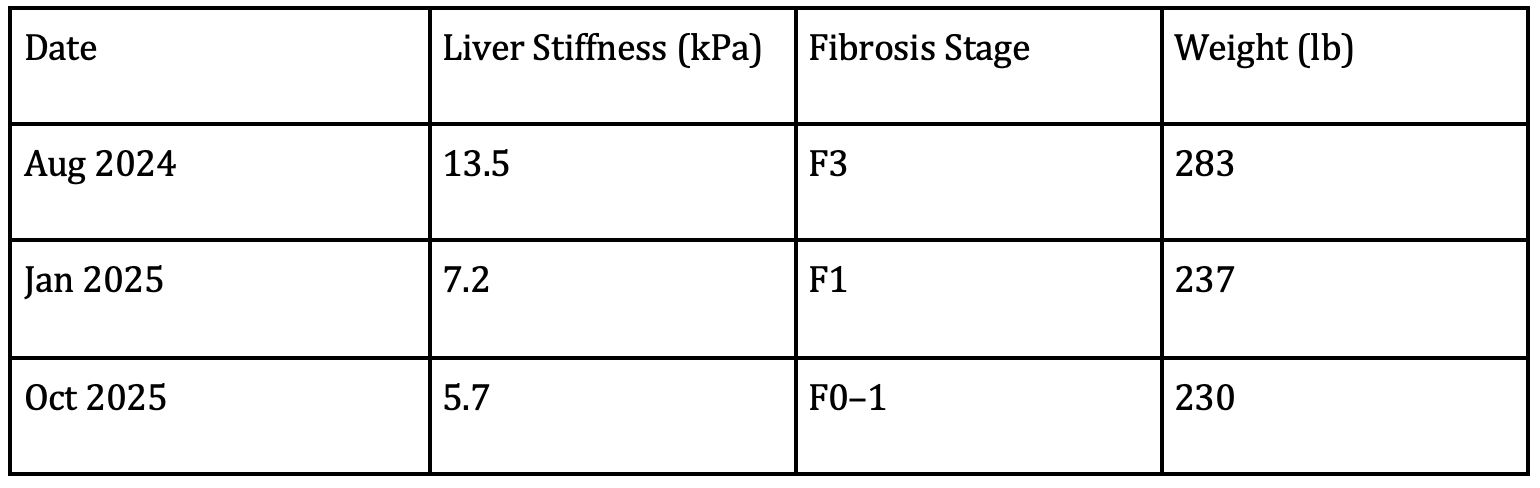
Serial transient elastography demonstrated progressive improvement in liver stiffness measurements. Liver stiffness decreased from 13.5 kPa at baseline (F3 fibrosis) to 7.2 kPa (F1 fibrosis) and subsequently to 5.7 kPa, corresponding to minimal fibrosis (F0–F1). These structural improvements occurred in parallel with metabolic recovery including weight loss and normalization of liver enzyme levels.
Serial laboratory measurements are summarized in Table 3 and FibroScan measurements in Table 4.
Table 3. Serial Metabolic and Biochemical Measurements
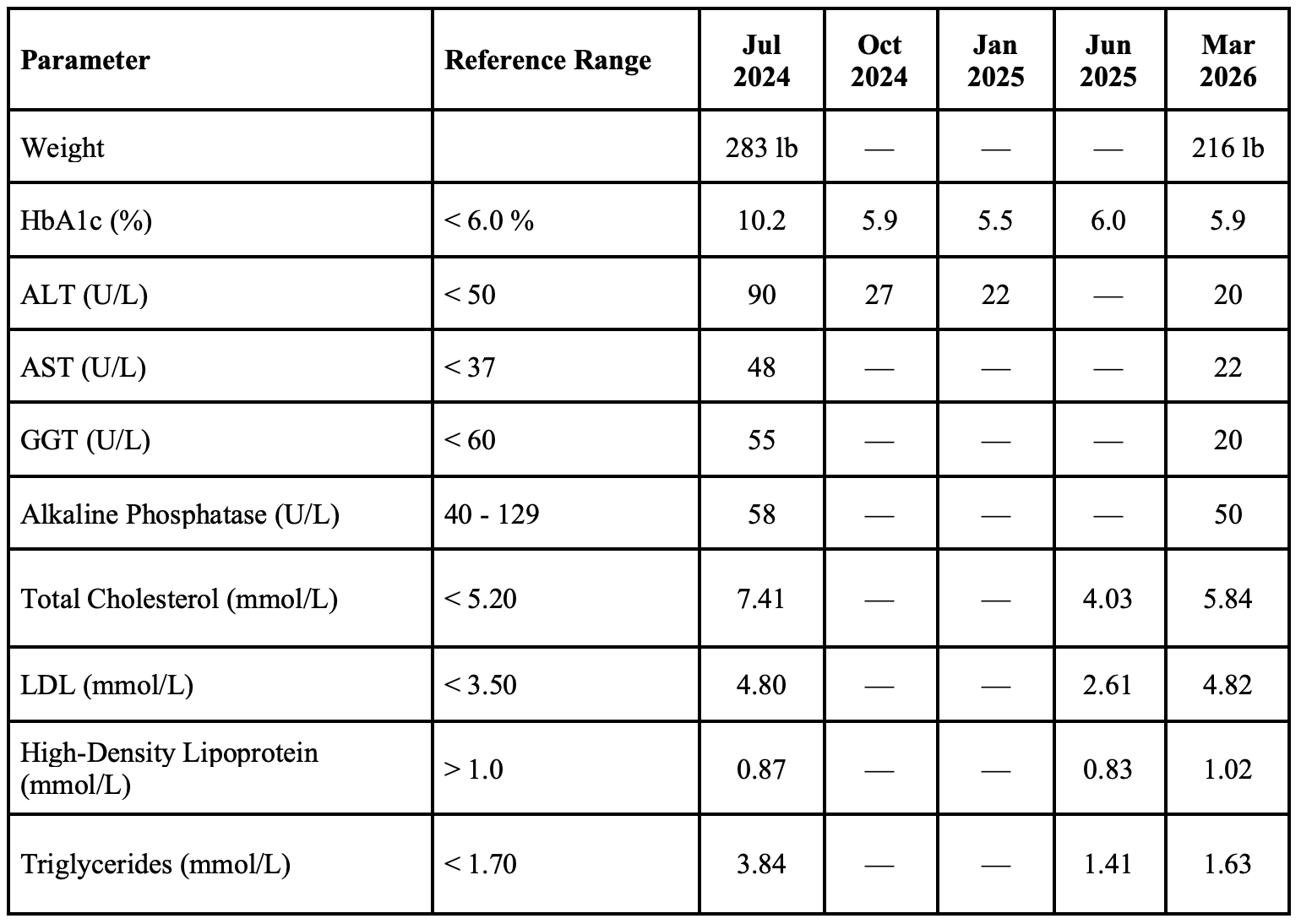
Table 4. FibroScan Progression
Discussion
The regression of hepatic fibrosis observed in this case occurred in the context of substantial metabolic improvement. There were notable corrections of several upstream drivers of hepatocellular injury with the implementation of a comprehensive orthomolecular treatment strategy. MASLD pathogenesis is closely linked to mitochondrial dysfunction, oxidative stress, and activation of hepatic stellate cells responsible for extracellular matrix deposition and progressive fibrosis (Friedman, 2008; Tilg & Moschen, 2010; Powell et al., 2021). Changes in liver stiffness of this magnitude on transient elastography are generally considered consistent with meaningful changes in hepatic fibrosis stage when accompanied by clinical and metabolic improvement (Powell et al., 2021).
Mitochondrial dysfunction is central to MASLD pathophysiology. Impaired β-oxidation of fatty acids leads to accumulation of lipotoxic intermediates and increased production of reactive oxygen species. Oxidative stress promotes hepatocellular injury and inflammatory signaling that ultimately activates fibrogenic pathways and stellate cell activation (Begriche et al., 2013; Sanyal et al., 2015; Tilg et al., 2021).
Activation of hepatic stellate cells represents a central event in hepatic fibrogenesis (Friedman, 2008; Kisseleva & Brenner, 2021). In response to hepatocellular injury and inflammatory signaling, stellate cells undergo phenotypic transformation into activated myofibroblast-like cells that produce extracellular matrix proteins including type I and type III collagen (Friedman, 2008). Progressive accumulation of collagen and other matrix components leads to architectural distortion of the liver and increasing fibrosis stage (Friedman, 2008; Kisseleva & Brenner, 2021). When the underlying drivers of hepatocellular injury are reduced, stellate cell activation may diminish and matrix remodeling pathways can permit partial regression of fibrosis (Kisseleva & Brenner, 2021).
Fibrosis regression is believed to occur when the balance between extracellular matrix deposition and degradation shifts toward matrix remodeling (Kisseleva & Brenner, 2021). Resolution of hepatic injury can reduce stellate cell activation while increasing activity of matrix metalloproteinases responsible for degradation of accumulated collagen (Kisseleva & Brenner, 2021; Powell et al., 2021). Experimental and clinical studies have demonstrated that under appropriate metabolic conditions hepatic fibrosis can partially regress through remodeling of the extracellular matrix and gradual resorption of fibrotic scar tissue (Kisseleva & Brenner, 2021; Powell et al., 2021).
Orthomolecular medicine seeks to restore optimal biochemical conditions required for cellular metabolism, emphasizing the role of micronutrients as enzymatic cofactors in mitochondrial respiration and antioxidant defense pathways (Ames, 2006; Begriche et al., 2013; Corbin & Zeisel, 2012). Micronutrients function as cofactors for numerous enzymatic reactions involved in mitochondrial respiration, antioxidant defense, and detoxification pathways. Restoration of micronutrient sufficiency may therefore support mitochondrial function and metabolic resilience, particularly in metabolic disorders characterized by impaired oxidative metabolism (Ames, 2006; Begriche et al., 2013).
Phosphatidylcholine plays an important role in hepatic lipid transport and membrane structure (Corbin & Zeisel, 2012; van der Veen, et al., 2017). Adequate phosphatidylcholine availability is required for assembly and secretion of very-low-density lipoproteins responsible for exporting triglycerides from hepatocytes (van der Veen et al., 2017). Impaired phosphatidylcholine availability has been associated with hepatic lipid accumulation and steatosis (Corbin & Zeisel, 2012; van der Veen, et al., 2017). Phospholipid support may therefore assist in reducing hepatic lipid accumulation and maintaining hepatocyte membrane integrity (Corbin & Zeisel, 2012).
A further mechanism relevant to orthomolecular therapy involves reduction of metal-catalyzed oxidative stress. Transition metals such as iron can catalyze the Fenton reaction, in which ferrous iron reacts with hydrogen peroxide to generate highly reactive hydroxyl radicals (Day & James, 1998; Begriche et al., 2013), as noted below:
Fe²⁺ + H₂O₂ → Fe³⁺ + OH⁻ + OH•
Hydroxyl radicals can induce lipid peroxidation, protein oxidation, and deoxyribonucleic acid damage within hepatocytes. Iron-catalyzed oxidative injury has been implicated in the progression of fatty liver disease and hepatic fibrosis (Day & James, 1998; Begriche et al., 2013; Powell et al., 2021).
EDTA chelation therapy forms stable complexes with several metal ions including iron and copper, thereby reducing their participation in catalytic oxidative reactions and representing one component of the broader strategy aimed at reducing oxidative stress. By binding redox-active metals, EDTA chelation therapy may reduce oxidative injury and inflammatory signaling within hepatic tissue (Begriche et al., 2013). Although the precise contribution of EDTA chelation therapy cannot be isolated in a single case, reduction of metal-mediated oxidative injury represents a biologically plausible mechanism supporting hepatic recovery.
Weight reduction and improvement in insulin sensitivity likely played a major role in this patient’s improvement. Sustained weight loss has been associated with histologic improvement and regression of fibrosis in metabolic liver disease (Armstrong et al., 2016; Powell et al., 2021). Metformin therapy was continued during treatment; however, metformin alone has not consistently demonstrated reversal of hepatic fibrosis in MASLD (Sanyal et al., 2015). The combined orthomolecular strategy addressing oxidative stress, mitochondrial function, membrane integrity, and micronutrient sufficiency may have contributed to the observed fibrosis regression.
Conclusion
This case demonstrates regression of advanced hepatic fibrosis in a patient with MASLD treated with a comprehensive metabolic and orthomolecular therapeutic approach. Improvement occurred in parallel with substantial metabolic recovery and normalization of liver enzyme levels.
Orthomolecular strategies targeting mitochondrial function, oxidative stress reduction, micronutrient sufficiency, membrane phospholipid support, and reduction of metal-catalyzed oxidative injury represent biologically plausible mechanisms contributing to hepatic recovery.
While causality cannot be established from a single case, the findings highlight the potential role of comprehensive metabolic restoration approaches in supporting reversal of liver injury in metabolic liver disease and support further investigation into orthomolecular strategies in MASLD management.
Ethics Statement
This case report was prepared in accordance with the CARE Case Report Guidelines. Written informed consent was obtained from the patient for publication of this de-identified case report. All identifying information has been removed or altered to protect patient privacy.
Conflict of Interest Statement
The author declares no conflicts of interest related to this case report.
Funding No external funding was received for preparation of this case report.
Author Contributions
Dr. Gannage conceived the clinical intervention, managed the case, and prepared the manuscript.
References
Armstrong, M. J., Gaunt, P., Aithal, G. P., Barton, D., Hull, D., Parker, R., Hazlehurst, J. M., Guo, K., LEAN trial team, Abouda, G., Aldersley, M. A., Stocken, D., Gough, S. C., Tomlinson, J. W., Brown, R. M., Hübscher, S. G., & Newsome, P. N. (2016). Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet (London, England), 387(10019), 679–690. https://doi.org/10.1016/S0140-6736(15)00803-X
Ames B. N. (2006). Low micronutrient intake may accelerate the degenerative diseases of aging through allocation of scarce micronutrients by triage. Proceedings of the National Academy of Sciences of the United States of America, 103(47), 17589–17594. https://doi.org/10.1073/pnas.0608757103
Begriche, K., Massart, J., Robin, M. A., Bonnet, F., & Fromenty, B. (2013). Mitochondrial adaptations and dysfunctions in nonalcoholic fatty liver disease. Hepatology (Baltimore, Md.), 58(4), 1497–1507. https://doi.org/10.1002/hep.26226
Corbin, K. D., & Zeisel, S. H. (2012). Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Current opinion in gastroenterology, 28(2), 159–165. https://doi.org/10.1097/MOG.0b013e32834e7b4b
Day, C. P., & James, O. F. (1998). Steatohepatitis: a tale of two “hits”?. Gastroenterology, 114(4), 842–845. https://doi.org/10.1016/s0016-5085(98)70599-2
Friedman S. L. (2008). Hepatic fibrosis — overview. Toxicology, 254(3), 120–129. https://doi.org/10.1016/j.tox.2008.06.013
Kisseleva, T., & Brenner, D. A. (2008). Mechanisms of fibrogenesis. Experimental biology and medicine (Maywood, N.J.), 233(2), 109–122. https://doi.org/10.3181/0707-MR-190
Powell, E. E., Wong, V. W., & Rinella, M. (2021). Non-alcoholic fatty liver disease. Lancet (London, England), 397(10290), 2212–2224. https://doi.org/10.1016/S0140-6736(20)32511-3
Sanyal, A. J., Friedman, S. L., McCullough, A. J., Dimick-Santos, L., American Association for the Study of Liver Diseases, & United States Food and Drug Administration (2015). Challenges and opportunities in drug and biomarker development for nonalcoholic steatohepatitis: findings and recommendations from an American Association for the Study of Liver Diseases-U.S. Food and Drug Administration Joint Workshop. Hepatology (Baltimore, Md.), 61(4), 1392–1405. https://doi.org/10.1002/hep.27678
Tilg, H., & Moschen, A. R. (2010). Evolution of inflammation in nonalcoholic fatty liver disease: the multiple parallel hits hypothesis. Hepatology (Baltimore, Md.), 52(5), 1836–1846. https://doi.org/10.1002/hep.24001
Tilg, H., & Effenberger, M. (2020). From NAFLD to MAFLD: when pathophysiology succeeds. Nature reviews. Gastroenterology & hepatology, 17(7), 387–388. https://doi.org/10.1038/s41575-020-0316-6
van der Veen, J. N., Kennelly, J. P., Wan, S., Vance, J. E., Vance, D. E., & Jacobs, R. L. (2017). The critical role of phosphatidylcholine and phosphatidylethanolamine metabolism in health and disease. Biochimica et biophysica acta. Biomembranes, 1859(9 Pt B), 1558–1572. https://doi.org/10.1016/j.bbamem.2017.04.006
Younossi, Z. M., Koenig, A. B., Abdelatif, D., Fazel, Y., Henry, L., & Wymer, M. (2016). Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology (Baltimore, Md.), 64(1), 73–84. https://doi.org/10.1002/hep.28431