Introduction
When cancer patients choose to undergo chemotherapy, often, they are aware that chemotherapy comes with side effects (Chemotherapy Side Effects, 2019, Nurgali K, et al, 2018) But because chemotherapy seems to be the only option available, patients, without questions, have come to accept the side effects of chemotherapy, while hoping that the prescribed therapy can prolong their lives further. However, what will happen if patients have more insight into cancer treatments? They may begin to understand the statistics underpinning chemotherapy treatments, and come to know that less well-known therapies, like nutritional therapy, exist. Nutritional therapy has begun to show an increasing promise in the treatment of many diseases, (Brighthope I, 2011, Levy T, 2019a, Levy T, 2019b) including cancer. (Brighthope I, 2011, Padayatty SJ, et al, 2006, Riordan HD, et al 2004, Yeom CH, et al, 2009, Vollbracht C, et al, 2011, Welsh JL, et al, 2013, Monti DA 2012)
An Overview on the Development of Cancer Guidelines
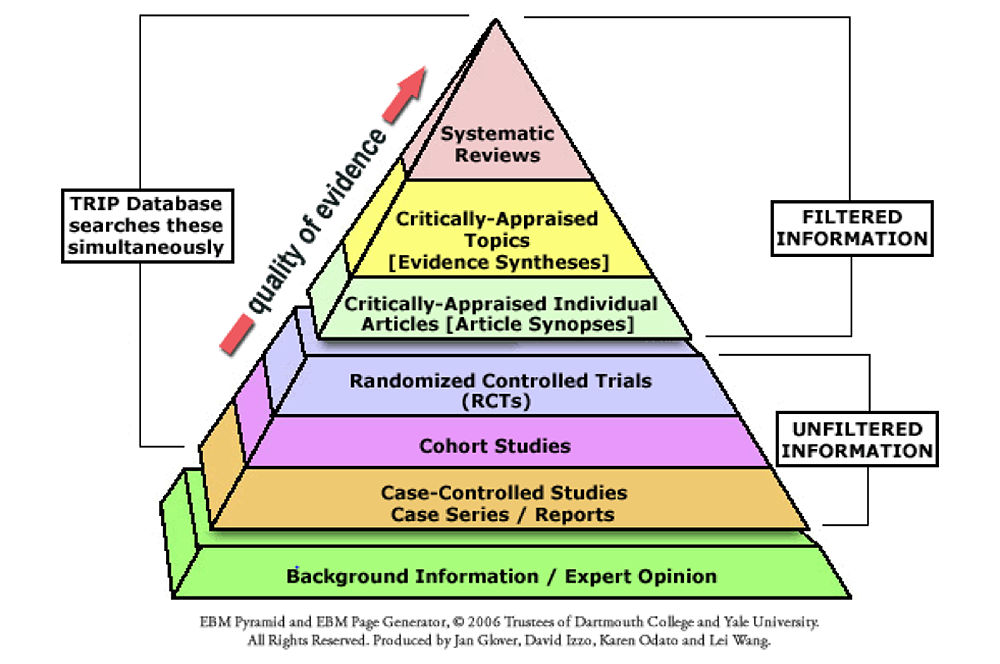
Clinical guidelines are recommendations that have been developed to help patients and doctors make the most appropriate medical decisions in the relevant clinical circumstance. They contain information to help doctors decide what would be the most appropriate treatments and diagnostic procedures for cancer. (Fadaka A et al, 2017) These recommendations are based on evidence from medical literature regarding cancer. However, there is a vast amount of medical literature written about cancer – some of them reliable and some of them not. (Umesh G, 2016) Therefore, a process is needed to help determine the reliability of these literature before they are being applied into clinical practice. (Umesh G, 2016). The evidence-based pyramid succinctly explains how the process works. (Liberti MV, Locasale JW 2016)
An Overview of the Drug-Approval Process
At the bottom of the pyramid is written observations of patients with outcomes of interest (Case studies/ case reports) (Evidence explained, 2019, Evidence-Based Practice, 2019) If there is indeed an interesting pattern going on with these case studies, for instance, when doctors notice that being exposed to Substance X was being associated with a decrease in tumour size, a cohort study will then be carried out. (Evidence explained, 2019, Evidence-Based Practice, 2019) The cohort study will then identify more people who have been exposed to Substance X and follow them to see if they also experience a decrease in their tumour size. (Evidence explained, 2019, Evidence-Based Practice, 2019) If indeed even more people prove to have a decrease in their tumour size after being exposed, then randomised controlled trials (RCTs) will be carried out. In RCTs patients are usually divided into two groups, one group will receive Substance X and one group will receive a placebo instead. (Chalmers TC, 1981) The patients will then be followed up to see if there is indeed a significant difference in outcome between the two groups. (Chalmers TC, 1981) Systematic reviews then look at all RCTs regarding the use of Substance X in the reduction of tumour size, compares it to other alternatives that are known to reduce tumour size, before making a statement on what would be the best alternative for shrinking tumours in cancer. (Evidence explained, 2019, Evidence-Based Practice, 2019) Clinical guidelines for the treatment of cancer are then based on systematic reviews.
Understanding how clinical guidelines are formulated is important because it shows how tightly linked clinical guidelines and clinical trials are. One could almost say that clinical guidelines are built on clinical trials. Therefore, how clinical trials are conducted can affect the clinical guidelines that are followed by medical systems around the world and consequently affect how cancer patients are being treated.
.
Conventional Cancer Treatments
(i) Flawed Clinical Trials
The example of Substance X will be used to further illustrate how cancer trials affect clinical guidelines. Since Substance X can reduce the size of tumours in cancer patients, researchers conducting RCTs of Substance X will try to prove this and the success of its clinical trial will be determined by how much of the tumour Substance X can shrink. It is important to note that Substance X’s ability to reduce the size of tumour is known as a surrogate endpoint in clinical trials19. Unlike the usual endpoint, a surrogate endpoint (e.g. tumour shrinkage) does not show a direct clinical benefit to patients, but rather it predicts how the usage of the drug would have effects that would benefit the patient. (Rothenberg ML, et al 1996, Lal R, 2019) A clear danger lies in the use of surrogate endpoints – they may not accurately predict clinical benefits, which is being defined as having a positive effect on the quality of life of the patient (being able to carry out activities of daily living) and increased overall survival rates of the individual. (Rothenberg ML, et al 1996,Lee JJ 2019, Group F-NBW 2018) This implies that Substance X although effective in reducing tumour size, may not necessarily allow patients to experience a prolonged survival time. (Moriwaki T, 2016, Blumenthal GM, 2015) Substance X, like most chemotherapy agents, could shrink tumours but also cause a suppression of immunity at the same time, putting patients at risk of infections and complications leading to an earlier death. (Suhaimi ND 2009, Vento S, 2003) This raises doubts on whether surrogate end points should be used to prove the efficacy of drugs in treating cancer.
Avastin is a good example of how the use of surrogate endpoints have fallen short. Avastin is a recombinant humanised antibody that has been indicated for use by the FDA on colorectal cancer, glioblastoma, metastatic renal cell carcinoma, ovarian and fallopian tube cancer and peritoneal cancer. (AVASTIN, bevacizumab) It works by binding to vascular endothelial growth factor (VEGF) so that VEGF does not interact with its receptors (Flt-1 and KDR) on the surface of endothelial cells, consequently inhibiting angiogenesis. (AVASTIN, bevacizumab) Progression-Free Survival (PFS) is the length of time a patient lives without progression of the disease after treatment and is also a surrogate endpoint. Avastin was initially approved to be used in combination with Paclitaxel in metastatic HER2-negative breast cancer for patients who had not received chemotherapy under the US FDA’s Accelerated Approval Program in February 22, 2008 because it showed an increase in PFS time by 5.5 years as compared to using Paclitaxel as a monotherapy in the E2100 trial. (Sasich LD, Sukkari SR, 2012, Kemp R, Prasad V, 2017) However this indication was withdrawn in 2011 after further trials (the AVADO and RIBBON 1 trials) failed to replicate an increase in PFS that was comparable in magnitude to the E2100 trial and participants being administered Avastin also experienced higher incidences of NCI CTC grade 3-5 adverse event and serious adverse events. (Sasich LD, Sukkari SR, 2012) In the RIBBON 1 trial, the rate of serious adverse events was almost twice as high in the bevacizumab arms compared to placebo arm. (Sasich LD, Sukkari SR, 2012)
PFS is a commonly used surrogate endpoint in cancer trials. It is therefore not unconceivable that if PFS backfired in Avastin, could they also not backfire in other cancer drug trials that utilise it as well? (Miessler J, 2018) These flawed trials then go on to be systematically reviewed and included into clinical guidelines which doctors follow in their treatment of cancer patients.
(ii) Off-Label Use of Chemotherapy Drugs
The conventional medical system places a strong emphasis on evidence-based medicine, as seen in the long and tedious process used to prove the clinical use of pharmacological drugs. However current clinical practice seems to be falling short of the evidence-based practice that the modern medical system is so proud of. Indicated use refers to the use of drugs to treat specific conditions that have been approved by governing bodies (like the US FDA) because of substantial evidence from drug trials proving that the drug is useful in treating that specific condition. (Natalia Mazina K, 2017) However, in certain situations, the drug is also useful in treating other conditions. Pharmaceutical companies may have chosen not to go through the long process of gathering evidence that it works for other conditions because of the cost and time involved. (Natalia Mazina K, 2017, Wittich CM 2012) Despite the lack of adequate evidence, doctors are legally allowed to prescribe an approved drug for uses not indicated in the prescription information (Day R, 2013, Handbook on Medical Ethics, 2016) They can do so as long as there is some level of evidence regarding the drug’s efficacy and the belief that doing so would be to the patient’s “best interest.” (Natalia Mazina K, 2017, Day R. 2019, Handbook on Medical Ethics 2016, Understanding Unapproved Use of Approved Drugs 2018). This is known as off-label prescription and is extremely common in oncology practice (Saiyed MM, 2017) when doctors run out of treatment options for their patient and off-label usage becomes part of a last effort to offer patients hope. (Understanding Unapproved Use of Approved Drugs 2018). Regardless, it does not deny that doctors may be going against their obligation to act in a non-maleficent way towards their patients. (Gupta SK, Nayak RP, 2014, Dressser R, 2009) Non-maleficence requires that the treatment benefits to outweigh the harms that may arise as result of undergoing treatment. Off-label prescription does not guarantee an efficacy in treating cancer and may in fact worsen patients’ health by weakening their immune systems, putting patients at risk of unnecessary infections. (Saiyed MM, 2017, Kang DH, et al, 2009, Cancer treatments, 2019, Beneficence and non-maleficence. 2019) One study looked at female patients aged 65 years and above, that were diagnosed with their first primary breast cancer between the years 2000-2007. (Eaton AA, et al, 2016) The study found that 64% of the treatment regimen prescribed had at least a chemotherapeutic agent that was not in line with the use indicated by FDA. (Eaton AA et al, 2016) Hospitalization/ER admission rate was also higher amongst patients undergoing regimens that consisted of chemotherapeutic agents not being indicated for use by the FDA, as compared to those that were undergoing regimens consistent with the use labelled by the FDA. (Eaton AA, et al, 2016) In view of the data, it is necessary rethink if prescribing off-label would truly be providing patients with more benefit than harm. In addition, off-label drugs are not always covered by medical insurance which means patients may have to pay for them out-of-pocket, putting themselves under unnecessary financial strain. (Saiyed MM, 2017, Yandall K, 2017) If more persuasion is needed regarding the harms that could occur from prescribing off-label, consider the case of Paroxetine. In 2001, Study 329 was being conducted to test the efficacy of Paroxetine in treating depression for young children. The result proved that Paroxetine was useful in treating depression and that formed the basis for off-label prescription of Paroxetine in adolescents. (Keller MB, et al, 2001) However further studies later indicated that Paroxetine actually increased suicide risk in these adolescents (Kondro W, Sibbald B, 2004) and from 2003 government agencies began to release warnings against the off-label prescriptions of Paroxetine in adolescents. (Kondro W, Sibbald B, 2004) Could this also not happen in oncology where off-label treatments put patients in a worse off position?
.
Alternatives
Oncologists tend to prescribe off label medications for their patients when they do not know what else they can do for their patients. However, are off-label chemotherapy drugs the only options that doctors truly have to offer? There are many other non-conventional therapies that are available for doctors to choose from – for instance high dose Vitamin C. High dose vitamin C was first proposed for the treatment of cancer by Linus Pauling (Nobel Prize winner) and Ewan Cameron in the 1970s. (Ewan C, Linus P. 1976, Cameron E, Pauling L, et al 1979) Both Pauling and Cameron were labelled quacks for their claims by the medical community after two flawed studies done by the Mayo Clinic, utilising oral vitamin C rather than intra-venous Vitamin C (IVC), presumably dispelled their credibility. (Creagan ET, Moertel CG,et al 1979, Moertel CG, Fleming TR, et al 1985) Extensive research in recent years, however, has shown immense potential in the use of high dose IVC for the treatment and support of cancer patients. High dose IVC has been shown to be selectively cytotoxic for cancer cells through the formation of hydrogen peroxide (Roomi MW, et al, 2016, Bram S, et al, 1980, Fujinaga S, et al, 1994, Gonzalez MJ, et al, 2005, Mastrangelo D, et al, 2015, l Banna N, et al, 2018, Raymond YCF, et al, 2016); reduces inflammation, (Lee WJ, et al, 2009, Mikirova N, et al, 2012, Mikirova N, et al, 2013, Ellulu MS, et al, 2015, Mikirova N, et al, 2016, Raymond YCF, et al, 2018) suppresses angiogenesis (a key factor in the spread and growth of cancer), (Yeom CH, et al, 2009, Mikirova NA, et al, 2008, Lee WJ, 2009, Raymond YCF, et al, 2018, Mikirova NA, et al, 2016) helps manage the symptoms arising from the use of chemotherapy drugs, (Riordan HD, et al, 2004, Vollbracht C, et al, 2011, Roomi MW, et al, 2016, Klimant E, 2018, Carr AC, et al 2014) increases quality of life for patients, (Vollbracht C, 2011, Carr AC, et al 2014, Takahashi H, et al, 2012, Chang HY, et al, 2007) safe for use with chemotherapy, (Vollbracht C, 2011, Welsh JL et al, 2013, Monti DA, 2012, Jung SA,2016) is safe in high doses (Raymond YCF, et al, 2016, Raymond YCF, et al, 2018, Jackson JA, et al, 2002, Schoenfeld JD, et al, 2017) and kills cancer stem cells. (Lv H, et al, 2018, Kim TJ, et al, 2018) Additionally, minimal side effects arise from the use of high dose IVC (Raymond YCF, et al, 2018, Stephenson CM, et al 2013, Jackson JA, et al 2002, High doses of vitamin C. 2019) and deaths due to the Vitamin C have yet to be reported between 2012-2017 in the US. (David D. et al 2018, Dovey D, 2014, David D 2016, James B 2015, James B. 2014, James B. 2012) Despite significant evidence indicating Vitamin C’s immense potential, majority of the mainstream medical community continues to argue against the use of IVC in patients undergoing chemotherapy on the basis that it is “non-evidence based” and ineffective. (Moertel CG, Fleming TR, et al 1985, Lee P. 2015, Unlu A, 2016)
.
Conclusion
(i) Do unto your patients as you would do unto yourself
The process underpinning conventional cancer treatment guidelines carries complexities, as discussed earlier, which patients may not necessarily be aware of. This is then added on to the stress and bewilderment patients face when they first receive their cancer diagnosis, when they are being swamped by information, test results, etc. Therefore, most patients rely on their doctor’s advice regarding conventional cancer therapy and then go on to follow their advice because it gives them the affirmation that they are doing the right thing. By prescribing conventional cancer therapies, medical professionals are discharging their expected duties. However, in situations like cancer, it may be more beneficial to the patient if the physician puts him or herself in the shoes of the patient and consider if they would carry out a similar treatment on themselves. Interestingly, a significant portion of medical professionals choose not to undergo conventional cancer therapy when diagnosed with cancer. (Mackillop WJ, et al, 1987, Lind SE, et al, 1991) Implementing more empathy into practice allows practitioners to rationalise what would be the best option for their patients and holds them to a standard where medical treatment is guided to maximise benefits for their patients rather than simply following standard protocols.
(ii) Keeping an Open Mind to Non-Conventional Cancer Treatments
The ideal cancer drug is one that is safe, effective, resistance free, cost effective with a large therapeutic window. Throughout the long history of conventional cancer research and treatment, it seems that these objectives have yet to be achieved. Mainstream cancer therapy continues to be heading in the opposite direction. Albert Einstein once said, “Insanity is doing the same thing over and over again and expecting different results”. It brings up the question as to whether conventional cancer therapy will continue to deliver the same limited outcomes in the future. Is it not time for the medical system to consider using alternatives like Vitamin C, which holds the potential to fulfil the role of an ideal cancer drug?
.
Acknowledgments
Funding: The authors did not receive any paid honoraria, financial support nor external grants for the authorship and/ or publication of this article from any pharmaceutical companies nor any other organizations.
Declaration of Conflicting Interests: The authors declare there are no conflicts of interest with respect to the research, authorship and/or publication of this article.
Authors contribution: Melissa H. was responsible for writing up on the flaws in clinical trials, off-label cancer drug use and compiling the references. Raymond Y. was responsible for the editing of the article, highlighting the use of off-label cancer drugs and providing references.
Special thanks: To all colleagues who have taken the time to review this paper.
.
References
AVASTIN (bevacizumab) – FDA. In: FDA, ed.
Blumenthal GM, Karuri SW, Zhang H, et al. Overall response rate, progression-free survival, and overall survival with targeted and standard therapies in advanced non-small-cell lung cancer: US Food and Drug Administration trial-level and patient-level analyses. Journal of Clinical Oncology. 2015;33(9):1008-1014.
Beneficence and non-maleficence.Alzheimer-europe.org. 2009; https://www.alzheimer-europe.org/Ethics/Definitions-and-approaches/The-four-common-bioethical-principles/Beneficence-and-non-maleficence. Accessed 2019 January 7.
Bram S, Froussard P, Jasmin C, et al. Vitamin C preferential toxicity for malignant melanoma cells. Nature. 1980;284(5757):629-631.
Brighthope I. Intravenous ascorbic acid in the treatment of influenza: Lack of evidence or incontrovertible ignorance? Journal of the Australian Traditional-Medicine Society. 2011(4):228.
Cameron E, Pauling L, Leibovitz B. Ascorbic Acid and Cancer: A Review. Cancer Research. 1979;39(3):663.
Cancer treatments can increase infection risk.Cancer.org. 2015;https://www.cancer.org/treatment/treatments-and-side-effects/physical-side-effects/infections/infections-in-people-with-cancer/how-treatment-increases-risk.html. Accessed January 23, 2019.
Carr AC, Vissers MCM, Cook J. Relief from cancer chemotherapy side effects with pharmacologic vitamin c. New Zealand Medical Journal. 2014;127(1388):66-70.
Chalmers TC, Smith Jr H, Blackburn B, et al. A method for assessing the quality of a randomized control trial. Controlled Clinical Trials. 1981;2(1):31-49.
Chang HY, Gyou CJ, Keun JS. Changes of terminal cancer patients’ health-related quality of life after high dose vitamin C administration. Journal of Korean Medical Science. 2007;22(1):7-11.
Chemotherapy Side Effects.Cancer.org. 2016 https://www. cancer.org/treatment/treatments-and-side-effects/treatment-types/chemotherapy/chemotherapy-side-effects. html. Accessed January 21, 2019
Clinical Trial Endpoints.Focr.org. https://www.focr.org/clinical-trial-endpoints. Accessed December 17, 2018.
Creagan ET, Moertel CG, O’Fallon JR, et al. Failure of High- Dose Vitamin C (Ascorbic Acid) Therapy to Benefit Patients with Advanced Cancer: A Controlled Trial. New England Journal of Medicine. 1979;301(13):687-690.
David D. Gummin JBM, Daniel A. Spyker, Daniel E. Brooks, Michael O. Fraser, William Banner. 2016 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 34th Annual Report. In: Clinical Toxicology; 2016.
David D. Gummin JBM, Daniel A. Spyker, Daniel E. Brooks, Krista M. Osterthaler and William Banner 2017 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 35th Annual Report. In: American Association of Poison Control Centers; 2018.
Day R. Off-label prescribing.nps.org. 2013; https://www.nps. org.au/australian-prescriber/articles/off-label-prescribing -6. Accessed Dec 27 2019.
Dovey D. Vitamin Overdose: Taking Too Many Vitamins Can Be Bad For Your Health, But How Many Would It Take To Kill You?Sciencedaily.com. 2014; https://www.medicaldaily.com/vitamin-overdose-taking-too-many-vitamins-can-be-bad-your-health-how-many-would-it-315426. Accessed 15 January, 2018.
Dresser R, Frader J. Off-Label Prescribing: A Call for Heightened Professional and Government Oversight. In: 2009: 476.
Eaton AA, Sima CS, Panageas KS. Prevalence and Safety of Off-Label Use of Chemotherapeutic Agents in Older Patients With Breast Cancer: Estimates From SEER-Medicare Data. Journal of the National Comprehensive Cancer Network : JNCCN. 2016;14(1):57-65.
El Banna N, Hatem E, Heneman-Masurel A, et al. P-371-Investigating redox-based anticancer mechanisms of vitamin C. Free Radical Biology & Medicine. 2018;120:S157-S157.
Ellulu MS, Rahmat A, Patimah I, Khaza’Ai H, Abed Y. Effect of vitamin C on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: A randomized controlled trial. Drug Design, Development and Therapy. 2015;9:3405-3412.
Evidence explained.Library.qut.edu.au. https://www.library. qut.edu.au/search/howtofind/evidencebased/evidenceexplained.jsp. Accessed January 22, 2019.
Evidence-Based Practice: Evidence Pyramid.Amedd. libguides.com.https://amedd.libguides.com/c. php?g=476751&p=3259492. Accessed January 2 2019.
Fadaka A, Ajiboye B, Ojo O, Adewale O, Olayide I, Emuowhochere R. Biology of glucose metabolization in cancer cells. Journal of Oncological Sciences. 2017;3(2):45-51.
Fujinaga S, Sakagami H, Kuribayashi N, et al. Possible Role of Hydrogen Peroxide in Apoptosis Induction by Ascorbic Acid in Human Myelogenous Leukemic Cell Lines. The Showa University Journal of Medical Sciences. 1994;6(2):135-144.
Gonzalez MJ, Miranda-Massari JR, Mora EM, et al. Orthomolecular oncology review: ascorbic acid and cancer 25 years later. Integrative Cancer Therapies. 2005(1):32.
Group F-NBW. BEST (biomarkers, endpoints, and other tools) resource. 2016; https://www.ncbi.nlm.nih.gov/ books/NBK453484/. Accessed December 25 2018.
Gupta SK, Nayak RP. Off-label use of medicine: Perspective of physicians, patients, pharmaceutical companies and regulatory authorities. Journal of Pharmacology & Pharmacotherapeutics. 2014;5(2):88-92.
Handbook on Medical Ethics In. 2016 ed. Singapore: Sinagpore Medical Council 2016:55.
High doses of vitamin C to improve cancer treatment passes human safety trial.Sciencedaily.com. 2017 https://www. sciencedaily.com/releases/2017/03/170330142341.htm. Accessed January 15, 2019.
Jackson JA, Riordan HD, Bramhall NL, Neathery S. Sixteen-Year History with High Dose Intravenous Vitamin C Treatment for Various Types of Cancer and Other Diseases. Journal of Orthomolecular Medicine, 2002;17(2):117-119.
James A. Jackson HDR, Nancy L. Bramhall, Sharon Neathery. Sixteen-Year History with High Dose Intravenous Vitamin C Treatment for Various Types of Cancer and Other Diseases Journal of Orthomolecular Medicine. 2002;17(2).
James B. Mowry DAS, Louis R. Cantilena, Elise Bailey, Marsha Ford 2012 Annual Report of the American Association of Poison Control Centers ’ National Poison Data System (NPDS): 30th Annual Report 2012.
James B. Mowry DAS, Louis R. Cantilena JR, Naya Mcmillan , Marsha Ford. 2013 Annual Report of the American Association of Poison Control Centers ’ National Poison Data System (NPDS): 31st Annual Report 2013.
James B, Mowry DAS, Daniel E. Brooks, Naya Mcmillan, Jay L. Schauben 2014 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 32nd Annual Report. In: Clinical Toxicology; 2014
James B. Mowry DAS, Daniel E. Brooksd, Ashlea Zimmermane, Jay L. Schaubenf. 2015 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 33rd Annual Report. In: Department of Medical Toxicology; 2015.
Jung S-A, Lee D-H, Moon J-H, et al. Original Contribution: L-Ascorbic acid can abrogate SVCT-2-dependent cetuximab resistance mediated by mutant KRAS in human colon cancer cells. Free Radical Biology and Medicine. 2016;95:200-208 Kang D-H, Weaver MT, Park N-J, Smith B, McArdle T, Carpenter J. Significant impairment in immune recovery after cancer treatment. Nursing Research. 2009;58(2):105-114.
Keller MB, Ryan ND, Strober M, et al. Efficacy of Paroxetine in the Treatment of Adolescent Major Depression: A Randomized, Controlled Trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2001(7).
Kemp R, Prasad V. Surrogate endpoints in oncology: when are they acceptable for regulatory and clinical decisions, and are they currently overused? BMC Medicine. 2017(1).
Kim TJ, Byun J-S, Kwon HS, Kim D-Y. Cellular toxicity driven by high-dose vitamin C on normal and cancer stem cells. Biochemical And Biophysical Research Communications. 2018;497(1):347-353.
Klimant E, Wright H, Rubin D, Seely D, Markman M. Intravenous vitamin C in the supportive care of cancer patients: A review and rational approach. Current Oncology. 2018;25(2):139-148.
Kondro W, Sibbald B. Drug company experts advised staff to withhold data about SSRI use in children. CMAJ : Canadian Medical Association Journal. 2004;170(5):783.
Ewan C, Linus P. Supplemental Ascorbate in the Supportive Treatment of Cancer: Prolongation of Survival Times in Terminal Human Cancer. Proceedings of the National Academy of Sciences of the United States of America. 1976;73(10):3685.
Lal R. “FDA Facilitates the Use of Surrogate Endpoints in Drug Development” November 5, 2018 Issue.Fda.gov. 2018 https://www.fda.gov/Drugs/DevelopmentApprovalProcess/SmallBusinessAssistance/ucm625076.htm. Accessed January 10, 2019
Lee JJ. Defining Clinical Benefit in Clinical Trials: FDA Perspective.Celiac.org. https://celiac.org/main/wp-content/ uploads/2015/04/great3-07.pdf. Accessed January 3, 2019.
Lee WJ. The prospects of vitamin C in cancer therapy. Immune Network. 2009;9(5):147-152.
Lee P. Provision of Intravenous Infusion of Vitamins, Glutathione And Hormonal Therapy In Licensed Healthcare Institutons. Singapore MoH, ed. Singapore 2015.
Levy T. The never-ending war against vitamin C. Peakenergy.com. 2016 https://www.peakenergy.com/articles/ nh20160314/The-never-ending-war-against-vitamin-C/. Accessed January 5 2019.
Levy T. The Clinical Impact of Vitamin C: My Personal Experiences as a Physician.Orthomolecular.org. 2016; http://orthomolecular.org/resources/omns/v10n14.shtml. Accessed January 3 2019 Nurgali K, Jagoe RT, Abalo R. Editorial: Adverse Effects of Cancer Chemotherapy: Anything New to Improve Tolerance and Reduce Sequelae? Frontiers in pharmacology. 2018;9:245-245.
Liberti MV, Locasale JW. The Warburg Effect: How Does it Benefit Cancer Cells? Trends in Biochemical Sciences. 2016;41(3):211-218.
Lind SE, Good MJD, Minkovitz CS, Good BJ. Oncologists vary in their willingness to undertake anti-cancer therapies. British Journal of Cancer. 1991;64(2):391-395.
Lv H, Wang C, Fang T, et al. Vitamin C preferentially kills cancer stem cells in hepatocellular carcinoma via SVCT- 2. npj Precision Oncology. 2018;2(1):1.
Mackillop WJ, Ward GK, O’Sullivan B. Non-small cell lung cancer: how oncologists want to be treated. International Journal of Radiation Oncology, Biology, Physics. 1987;13(6):929-934.
Mastrangelo D, Massai L, Lo Coco F, et al. Cytotoxic effects of high concentrations of sodium ascorbate on human myeloid cell lines. Annals of Hematology. 2015(11):1807.
Miessler J. Cancer Trials: Is Progression-Free Survival Enough? Centerwatch.com. 2018 https://www.centerwatch.com/cwweekly/2018/10/08/cancer-trials-is-progression-free-survival-enough/. Accessed January 10, 2019.
Mikirova NA, Ichim TE, Riordan NH. Anti-angiogenic effect of high doses of ascorbic acid. Journal of Translational Medicine. 2008;6:50-50.
Mikirova N, Casciari J, Rogers A, Taylor P. Effect of high-dose intravenous vitamin C on inflammation in cancer patients. Journal of Translational Medicine. 2012;10:189-189.
Mikirova N, Casciari J, Riordan N, Hunninghake R. Clinical experience with intravenous administration of ascorbic acid: achievable levels in blood for different states of inflammation and disease in cancer patients. Journal of Translational Medicine. 2013;11(1):1-10.
Mikirova N, Riordan N, Casciari J. Modulation of Cytokines in Cancer Patients by Intravenous Ascorbate Therapy. Medical science monitor : International Medical Journal of Experimental and Clinical Research. 2016;22:14-25.
Mikirova NA, Casciari JJ, Riordan NH. Ascorbate inhibition of angiogenesis in aortic rings ex vivo and subcutaneous Matrigel plugs in vivo. Journal of Angiogenesis Research. 2010;2:2-2.
Monti DA, Mitchell E, Bazzan AJ, et al. Phase I evaluation of intravenous ascorbic acid in combination with gemcitabine and erlotinib in patients with metastatic pancreatic cancer. Plos One. 2012;7(1):e29794-e29794.
Moertel CG, Fleming TR, Creagan ET, Rubin J, O’Connell MJ, Ames MM. High-Dose Vitamin C versus Placebo in the Treatment of Patients with Advanced Cancer Who Have Had No Prior Chemotherapy. New England Journal of Medicine. 1985;312(3):137-141.
Moriwaki T, Yamamoto Y, Kobayashi M, et al. Correlations of survival with progression-free survival, response rate, and disease control rate in advanced biliary tract cancer: A meta-analysis of randomised trials of first-line chemotherapy. British Journal of Cancer. 2016;114(8):881-888.
Natalia Mazina K, Hockel, Iezza, Patel. Recent Developments in Off-Label Use and Legal Implications to Physicians.Americanbar.org. https://www.americanbar. org/groups/health_law/publications/aba_health_esource/2016-2017/november2017/offlabeluse/. Accessed February 1 2019.
Padayatty SJ, Katz A, Levine M, Hewitt SM, Hoffer LJ, Riordan HD. Intravenously administered vitamin C as cancer therapy: Three cases. CMAJ. 2006;174(7):937-942.
Raymond YCF, Glenda CSL, Meng LK. Effects of High Doses of Vitamin C on Cancer Patients in Singapore: Nine Cases. Integrative Cancer Therapies. 2016;15(2):197-204.
Raymond YCF, See M, Loke SA, Wei YT. High-Dose Vitamin C Helps Prevent Recurrence of Stage IV Ovarian Cancer: A Case Report. Journal of Orthomolecular Medicine. 2018;33(4).
Riordan HD, Riordan NH, Jackson JA, et al. Intravenous vitamin C as a chemotherapy agent: a report on clinical cases. Puerto Rico Health Sciences Journal. 2004; 23(2): 115-118.
Roomi MW, Shanker N, Niedzwiecki A, Rath M. Vitamin C in Health: Scientific focus on its anti-cancer efficacy. Cellular Medicine and Natural Health Journal June 15 2016.
Rothenberg ML, Burris Iii HA, Von Hoff DD, et al. A phase II trial of gemcitabine in patients with 5-FU-refractory pancreas cancer. Annals of Oncology. 1996;7(4):347-353.
Saiyed MM, Ong PS, Chew L. Off-label drug use in oncology: a systematic review of literature. Journal of Clinical Pharmacy and Therapeutics. 2017(3):251.
Sasich LD, Sukkari SR. The US FDAs withdrawal of the breast cancer indication for Avastin (bevacizumab). Saudi pharmaceutical journal : SPJ : the official publication of the Saudi Pharmaceutical Society. 2012;20(4):381-385.
Schoenfeld JD, Sibenaller ZA, Mapuskar KA, et al. O(2) (?-) and H(2)O(2)-Mediated Disruption of Fe Metabolism Causes the Differential Susceptibility of NSCLC and GBM Cancer Cells to Pharmacological Ascorbate. Cancer Cell. 2017;31(4):487-500.e488.
Stephenson CM, Levin RD, Spector T, Lis CG. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemotherapy and Pharmacology. 2013;72(1):139-146.
Suhaimi ND. Infection after chemotherapy led to death. The Sunday Times, 2009.
Takahashi H, Mizuno H, Yanagisawa A. Original article: High-dose intravenous vitamin C improves quality of life in cancer patients. Personalized Medicine Universe. 2012;1:49-53.
Umesh G, Karippacheril JG, Magazine R. Critical appraisal of published literature. Indian Journal of Anaesthesia, 2016;60(9):670-673.
Understanding Unapproved Use of Approved Drugs “Off Label”.fda.gov. https://www.fda.gov/forpatients/other/offlabel/default.htm. Accessed January 13, 2018
Unlu A, Kirca O, Ozdogan M, Nayır E. Review: High-dose vitamin C and cancer. Journal of Oncological Science. 2016;1:10-12.
Vento S, Cainelli F. Infections in patients with cancer undergoing chemotherapy: aetiology, prevention, and treatment. Lancet Oncology. 2003(10):595.
Vollbracht C, Weiss G, Schneider B, Auerbach L, Leendert V, Beuth J. Intravenous vitamin C administration improves quality of life in breast cancer patients during chemo-/ radiotherapy and aftercare: Results of a retrospective, multicentre, epidemiological cohort study in Germany. In Vivo. 2011;25(6):983-990.
Welsh JL, Wagner BA, van’t Erve TJ, et al. Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer (PACMAN): results from a phase I clinical trial. Cancer Chemotherapy and Pharmacology. 2013(3):765.
Wittich CM, Burkle CM, Lanier WL. Ten common questions (and their answers) about off-label drug use. Mayo Clinic proceedings. 2012;87(10):982-990.
Yandall K. Going Off-Label.Cancertodaymag.org. 2017; https://www.cancertodaymag.org/Pages/Summer2017/ Going-Off-Label-Targeted-Therapy-Immunotherapy. aspx.
Yeom CH, Lee G, Park J-H, et al. High dose concentration administration of ascorbic acid inhibits tumor growth in BALB/C mice implanted with sarcoma 180 cancer cells via the restriction of angiogenesis. Journal of Translational Medicine. 2009;7:70-70